
 Medically Reviewed
Medically Reviewed
Key Takeaways
- “Skinny fat” describes a look where weight is lower but muscle is lacking, resulting in a softer, less defined appearance.
- Rapid weight loss with tirzepatide can lead to muscle loss if calorie intake is too low.
- Adequate protein intake, typically 1.2 to 2.2 g/kg, helps preserve muscle during a calorie deficit.
- Resistance training signals your body to retain muscle, supporting better shape and strength as you lose weight.
- Tracking intake and weight helps keep your calorie deficit controlled and aligned with sustainable progress.
Millions of people all over the world are using GLP-1s, like semaglutide and tirzepatide, to lose impressive amounts of weight. But what happens when you’ve been on tirzepatide for months, the scale is way down, and you’re not happy with how you look in the mirror?
“Skinny fat” isn’t a new label, but it’s seeing a resurgence as GLP-1s continue to grow in popularity. It describes a disconnect between the quantity of weight loss and the quality of what’s left behind.
If your body feels as droopy as the oversized clothing you no longer wear, you need to know how to prevent skinny fat on tirzepatide—or manage it if it’s already happened. This guide will explain the science behind the “skinny fat” phenomenon and teach you how to combat it.
What Is “Skinny Fat”?
According to Google Trends, skinny fat has been a recognized part of our health lexicon since at least 2004 and peaked in the mid-2010s. But as GLP-1s continue to surge in popularity, it’s coming back into vogue.
Skinny fat describes a particular look: a slender, average-sized silhouette, but loose, flabby, or under-muscled. Skinny-fat “symptoms” can be concealed under clothing, but loose skin and sparse muscle mass may deter you from disrobing.
Before we proceed, it’s essential to understand that self-image is a nuanced and multifaceted topic. Research tells us that, while weight loss tends to correlate with improved self-image, it’s not a silver bullet—even bodybuilders with lean, vascular physiques struggle with self-perception.
More importantly:
- “Skinny fat” is not a recognized medical condition. It’s an informal, and in some cases derogatory, aesthetic descriptor for a particular look.
- GLP-1s do not directly affect muscle. Skinny fat occurs as a consequence of conscious health decisions, but may be exacerbated if you’re on a GLP-1 like tirzepatide.
- Being skinny fat says nothing about your worth as a human being, nor is it an indicator of laziness or gluttony. It’s okay to want to change how you look, but if tirzepatide is helping you reclaim your health, being skinny fat pales in comparison.
That said, preventing skinny fat on tirzepatide is all about understanding how it occurs in the first place.
How Skinny Fat Happens on Tirzepatide
GLP-1s like tirzepatide and semaglutide encourage weight loss by regulating how much you feel like eating, and how full you stay after a meal. There are other mechanisms at play, but the result is clear: Data tell us that people using tirzepatide for a year or more lose about 20% of their body weight on average.
For heavily overweight or obese individuals, large weight loss transformations can be life-saving. However, there are side effects—including, in some cases, ending up skinny fat.
Do GLP-1s Make You Skinny Fat?
The short answer? No, GLP-1s do not make you skinny fat, but it can be a downstream consequence. Tirzepatide and its cousins encourage weight loss by regulating appetite, leading to significant, and often rapid, changes in body composition.
Appetite Suppression & Energy Balance
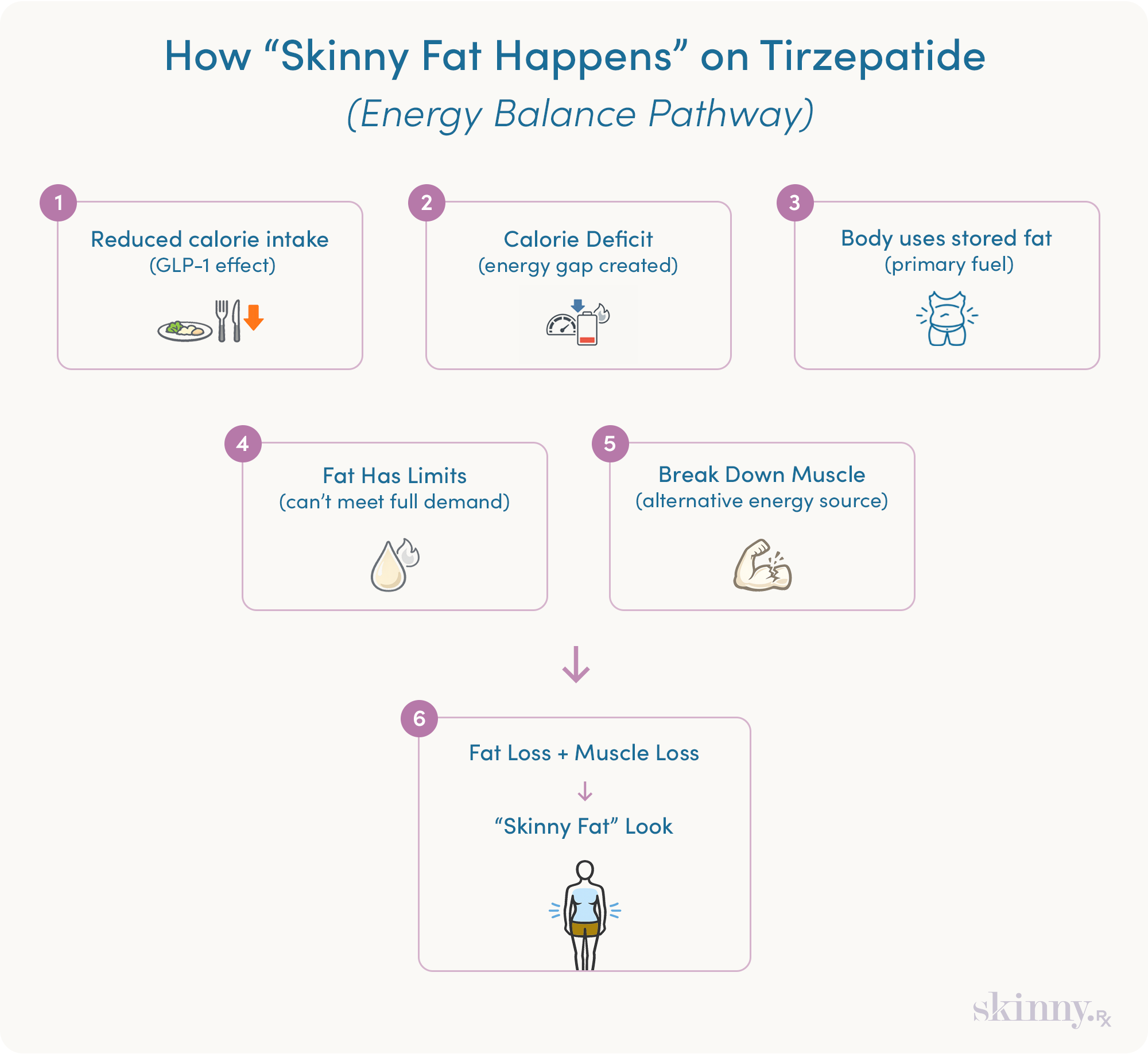
Eating too little, for too long, as a result of tirzepatide’s appetite-suppressing effects, can lead to skinny fat. How? By throwing your body’s “balance sheet” out of whack. Here’s how it works:
- Reducing your calorie intake creates a calorie deficit.
- To cover your energetic expenses (workouts, general movement), your body draws from its savings account—stored fat.
- Your body can only oxidize fat (convert stored fat into usable energy) so fast.
- If your energy needs are too high to be covered with fat oxidation, your body will harvest other sources, like muscle, to make up the difference.
Researchers have stated that weight loss of more than 10% in 6 months may come with health risks, including the loss of muscle as well. The Mayo Clinic regards losing two pounds per week as a “soft ceiling” for safe weight loss.

A Better Way to Lose Weight
Take a quick assessment to see if tirzepatide is right for you, and get a weight-loss plan built around your body, your goals, and long-term results.
The Critical Role of Strength Training
The adage “use it or lose it” applies: If you don’t give your body a reason to keep its muscle tissue, it’s at risk of being cannibalized for energy. This is why exercise routines are commonly prescribed alongside weight loss interventions like GLP-1s.
Physical activity burns calories and can help you achieve an energy deficit if you’re sedentary. But if you’re on your feet all day or work a laborious job, hitting the gym may not be necessary to kickstart weight loss once you’ve reduced your caloric intake.
That said, working out—particularly strength training, which targets your skeletal muscles more than your cardiovascular system—gives your body a justification to maintain its muscle mass. This is also why resistance training is commonly prescribed for the elderly. Lifting weights can delay or even halt muscle loss.
Preventing Skinny Fat on Tirzepatide: The 3 Pillars
Eating too little and not lifting weights can cause your body to shed both fat and muscle over time. Skinny fat isn’t strictly caused by tirzepatide, but if you want to avoid it, you’ll need to stick to these three pillars.
Calorie & Protein Intake: Calibration Matters
GLP-1s like tirzepatide naturally discourage you from eating, which puts you in a calorie deficit. The problem? If you aren’t tracking your intake in some way, you can’t be sure just how deep that deficit is. To be sure, you’ll want to gather data from both sides by tracking your nutritional intake and weight changes.
- Caloric Intake: You should have, at least, a consistent ballpark figure of how many calories you’re eating each day. You can do this by sticking to a meal plan with consistent food sources, or by tracking calories in an app or on paper. Remember, clinical data and industry rules of thumb regard the conservative ceiling for “safe” weight loss around two pounds on the scale per week, or 1% of total body weight lost per week—whichever is lower. In practice, that works out to a 1,000-per-day calorie deficit at most.
- Protein: In times of great need, your body can convert amino acids (the building blocks of muscle tissue) into energy via a process called gluconeogenesis. Eating more protein can help mitigate this when you’re in a calorie deficit. How much? Recommendations vary, but research on protein intake for tirzepatide users indicates a range of 1.2 to 2 grams per kilogram of body weight per day. If you perform strength training workouts regularly, you can benefit from higher ranges of 1.6 to 2.2.
Body Composition Tracking: Scales vs. Scans
Once you’ve got a handle on how much is coming in, you can measure it against your rate of weight loss. Regularly stepping on the scale is the most straightforward method, even though it provides an incomplete picture and may be intimidating for some people.
- Scales tell you how much weight you’re losing, not what the weight is made of. Standard scales can’t differentiate between fat, muscle, water weight, undigested food in your stomach, or discount the clothes you’re wearing.
- More precise methods of assessing body composition, like scanners, exist. However, they’re not diagnostically perfect and can be expensive to access.
The simplest method is to weigh yourself regularly. You can reduce “signal noise” in the data by stepping on the scale in the morning, naked, after a bowel movement but before eating, either daily or once a week.
If you can find and afford body composition scanning, you may get more specific information, but it’s certainly not required.
Resistance Training: Non-Negotiable
Hitting the weights isn’t an exercise in vanity; it’s a countermeasure against the metabolic consequences of muscle loss. Resistance training also happens to be an excellent deterrent against skinny fat.
Maintaining or building muscle curtails skinny fat by “scaffolding” fat and loose skin, giving it something to cling to and maintain its shape. Having more muscle improves shape and firmness, and may even help skin recover some of its tautness.
Is it an aesthetic choice? Sure, but that’s just the icing on the cake. Strength training is one of the highest return-on-investment activities you can do for general health & longevity, whether you’re using a GLP-1 or not.
Preventing Skinny Fat on Tirzepatide: Add-Ons That Work
Maintaining an appropriate calorie deficit, hitting the gym, and eating more protein are the core pillars of preventing skinny fat on tirzepatide. If you want to do a bit more, you have some options.
Creatine Monohydrate: Essential for GLP-1 Users?
You’ve probably heard of creatine before—a high-octane, steroid-adjacent supplement for meatheads. But creatine’s reputation could not be more divorced from its reality.
Creatine monohydrate powder isn’t a steroid, nor is it dangerous. Put simply, it mainly helps your muscles store and utilize more fuel and fluid, empowering muscle contractions and reducing fatigue.
Creatine is also one of the most thoroughly researched sports supplements out there, with decades of clinical data corroborating its safety and efficacy. Should you take creatine on GLP-1s? Maybe.
- Data on older, non-exercising people taking creatine shows that supplementation can delay muscle loss.
- We have similar findings in younger, active people as well, with findings showing creatine reduces muscle loss during a calorie deficit compared to placebo.
One caveat: Creatine causes you to hold more water, which may affect the readings you get from weighing yourself. This is where a body composition scan can come in clutch, but after a few weeks of using creatine, things should level out again.
Anti-Myostatin Therapies
There are also emerging treatments meant to target the mechanisms behind muscle loss on GLP-1s at the source. Preliminary studies from 2025 have shown that therapies targeting myostatin and other ligand receptors can curb muscle loss and potentially accelerate fat loss.
However, these interventions are both financially prohibitive for many people and in need of more thorough research. There’s promise, but anti-myostatin therapies are more like speculative biohacking than practical solutions.
A Better Way to Lose Weight
Take a quick assessment to see if tirzepatide is right for you, and get a weight-loss plan built around your body, your goals, and long-term results.
Final Thoughts
Preventing “skinny fat” on tirzepatide comes down to how you approach weight loss, not just how much you lose. Prioritize protein, avoid overly aggressive calorie cuts, and include resistance training to help preserve muscle as the scale moves down. You don’t need perfection or complexity, just consistency in the habits that shape how your results actually look and feel.
If you’re considering GLP-1s for weight loss, a guided assessment through SkinnyRx can help determine your eligibility, match you with an appropriate treatment plan, and provide ongoing clinical support as you work toward your goals.
Frequently Asked Questions

By Jake Dickson, NASM-CPT, USAW-L2
Contributing Author
Jake holds a B.S. in Exercise Science from UNC Wilmington and began his career as a personal trainer and weightlifting coach. In recent years, he’s moved behind the page as a writer and editor, contributing hundreds of articles and being featured as a subject matter expert. Today, Jake’s goal remains the same: to empower people to change their lives by bringing heady scientific topics down to ground level.


