
 Medically Reviewed
Medically Reviewed
Key Takeaways
- Body recomposition focuses on losing fat while preserving muscle, rather than chasing weight loss alone.
- GLP-1 medications reduce appetite, but rapid or aggressive calorie deficits increase the risk of muscle loss.
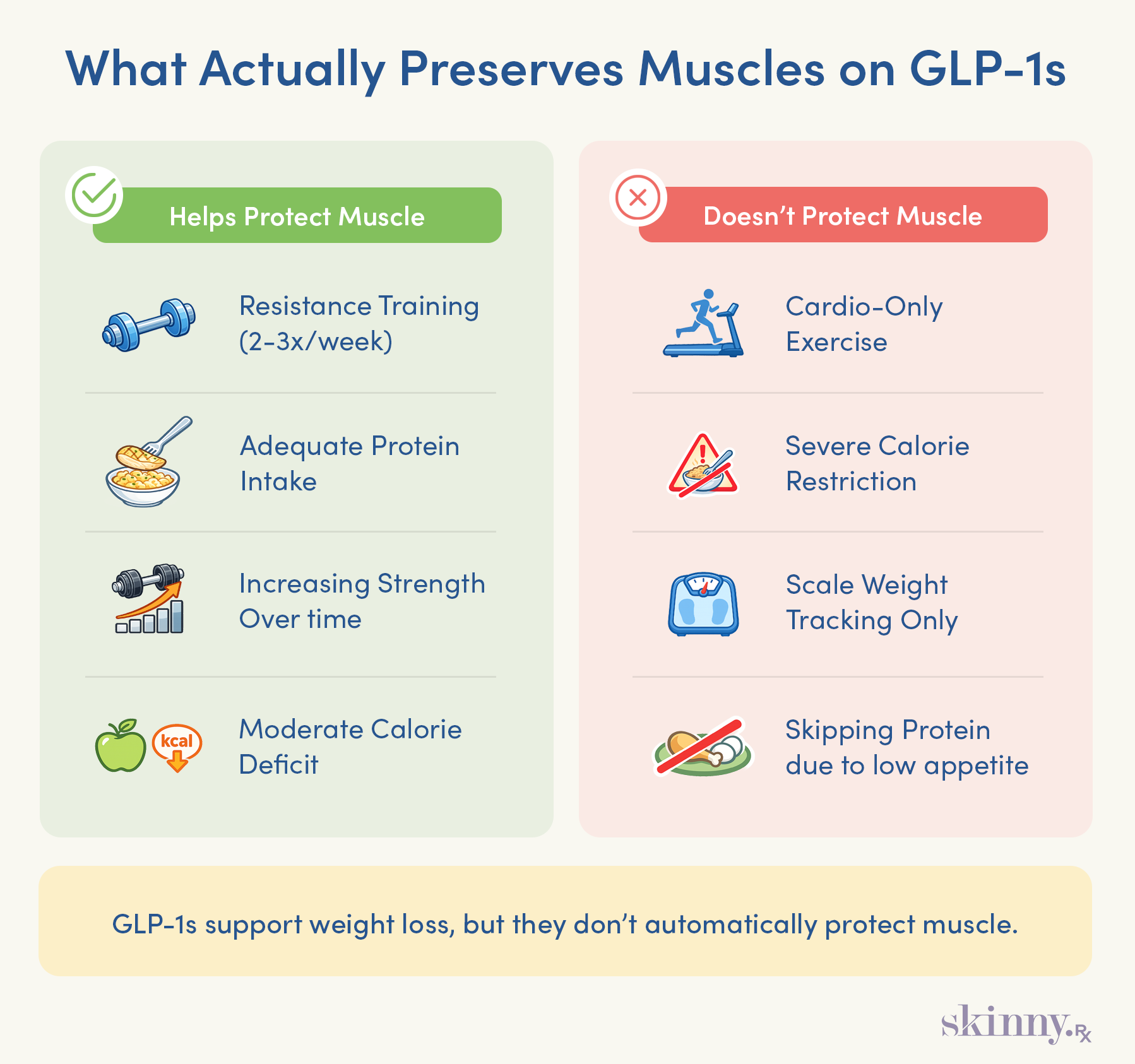
- Resistance training provides the strongest signal for the body to maintain muscle during weight loss.
- Higher protein intake is necessary during weight loss to support muscle repair and preservation when calories are reduced.
- The scale cannot distinguish fat loss from muscle loss, making strength, measurements, and health markers essential for tracking real progress.
When you’re trying to lose weight, it’s easy to fixate on the scale, but it can’t tell you what you’re losing or what kind of body you’re building along the way. The scale doesn’t distinguish between fat and muscle, and that distinction matters.
Muscle mass is a powerful predictor of longevity, supports bone density, improves metabolic health, and helps stabilize blood sugar. In short, how you lose weight matters just as much as how much you lose.
That’s where body recomposition comes in. Instead of chasing weight loss alone, body recomposition focuses on losing fat while maintaining, or even building, lean muscle. Two people can weigh the same and look and function very differently.
One may appear “skinny fat,” with low muscle and poorer metabolic health, while the other carries more muscle, burns more calories at rest, and moves with more stability.
GLP-1 medications are well-studied fat-loss tools, but they don’t automatically lead to a stronger physique. In fact, GLP-1 users risk losing between 40 and 60 percent of their lean mass (which also includes organs, bones, fluids, and even water stored in fat tissue).
When calories and appetite drop quickly, the body needs clear signals to keep muscle around. Without them, a meaningful portion of weight loss can come from lean mass.

Before starting any patient on a GLP-1 medication, I always explain how important it is to maintain their protein intake and keep up with resistance training. The goal is to hold onto your muscle while losing fat. If you can do that, you will improve your metabolism and overall health. That’s when you’ll really notice the difference: in how you feel, how your clothes fit, and in your lab work—things like blood sugar and cholesterol levels. Your scale won’t always move as much as you’d expect, but that’s not a bad sign. You’re changing your body’s composition and metabolism, which matters far more than the number on the scale.
–
Dr. Daniel McGee, Board-certified Family Medicine Physician
The Science of "Recomp": How to Burn Fat Without Losing Muscle
Weight loss requires a calorie deficit—meaning you burn more calories than you eat. You can get there by trimming calories, moving more, or both. When you’re in that deficit, your body pulls energy from two primary sources: carbohydrates and fat. Carbs are the quick fuel your body taps first, especially during exercise.
Once those stores run low, your body shifts to burning fat. But if your deficit is too aggressive (think: consistently cutting 500-plus calories a day), you increase your risk of losing muscle tissue.
Your body has a long daily to-do list, and some of those items are essential—running your organs, powering your brain, regulating temperature, rebuilding cells. When calories become scarce, hanging onto muscle is de-prioritized.
If you’re not eating enough to support those essential functions, your body may raid muscle tissue for amino acids to keep everything operating smoothly.
There are a few strategies you can employ to convince your body that your muscle is worth preserving. You need to signal to your body that it’s a necessity and provide enough “building blocks” so it doesn’t steal resources from your existing muscle. Here’s how to do that.
The Resistance Training Blueprint
The simplest and most effective way to stimulate your muscles is through resistance training. That load provides a new stressor to your muscle(s), which in turn respond by growing larger. Research has shown that resistance training while in a calorie deficit can preserve muscle tissue and simultaneously increase strength.
Strength Training Basics
You don’t need to push yourself to the limit, either. While some research has found that you can maintain muscle with as little as one all-out set per muscle per week, a general recommendation is to train each muscle twice per week for six total sets. Perform eight to 12 reps per exercise, and lift with moderate intensity; basically, you should feel like you can only do two more reps at the end of each set.
A good starting point is two full-body workouts a week. Aim for one pushing movement, one pull, one knee bend, one hip hinge, a loaded carry of sorts, and a core exercise. Here’s a quick list of options:
- Push: dumbbell bench press, push-up, dumbbell overhead press
- Pull: lat pulldown, inverted row, dumbbell row
- Knee Bend: split squat, walking lunge, goblet squat
- Hip Hinge: Romanian deadlift, kettlebell deadlift, kettlebell good morning
- Load Carry: farmer’s walk, kettlebell march
- Core Exercise: plank, russian twist, pallof press
Progressing your workouts is the true key to muscle retention. Your body is quick to adapt to new challenges, so you need to increase the intensity every session, or at least every week. The best way to progress is to add a small amount of weight—like the smallest amount your gym allows—or to do an extra rep.

Doctor-Guided Medical Weight Loss
Learn how prescription GLP-1 medications like semaglutide or tirzepatide may support weight loss when guided by a licensed medical provider and tailored to your health history.
The High-Protein Advantage
Protein isn’t just another macronutrient; it’s the raw material your body uses to build and maintain lean muscle tissue. When calories are low, protein becomes even more important because it helps stimulate muscle protein synthesis (MPS), the process responsible for repairing and preserving muscle. On GLP-1 medications, which suppress your appetite, hitting the right protein target helps ensure that most of the weight you lose comes primarily from fat.
Equally important to retaining muscle as you lose weight is to up your protein intake. The U.S. Recommended Daily Allowance is 0.36 grams per pound of body weight, or just 65 grams for a 180-pound person. That’s the amount needed to avoid a deficiency, but it’s generally considered too low for active adults.
How Much Protein Should You Eat?
If you’re lifting weights—which you should be to hang on to muscle tissue—you need protein so your body can complete its vital functions and tend to your muscle tissue. A paper published in the Academy of Nutrition and Dietetics suggests between 0.55 and 0.69 grams per pound of body weight.
To find your minimum target, multiply your body weight in pounds by 0.55. For a 180-pound person, that’s 100 grams of protein per day. Start there, and feel free to increase the amount of protein you’re eating up to a gram per pound of body weight. More than that won’t hurt, but it’s unnecessary.
When Should You Eat Your Protein?
The science isn’t settled on protein timing. However, there doesn’t seem to be a practical limit to how much protein your body can absorb and utilize from one meal. Hitting your overall protein goal for the day is more important than a per-meal quota. Still, nutrition experts recommend that you divvy up your protein goal evenly throughout the day.
For weight loss, when you eat is far less important than hitting your overall calorie target. Eat six small meals or two big ones—it doesn’t matter as long as you hit your calorie goals. However, users of semaglutide may have other nutritional priorities, such as blood sugar management and hunger control.
Eating three to five times a day (think: three meals and two snacks) can keep you satiated from morning to bedtime and ensure steadier blood sugar levels throughout the day. Though it’s important to note that if hunger isn’t an issue for you, there is some research that suggests as few as two to three meals can help with blood sugar control.
When it comes to maintaining muscle mass, some studies also show that eating even one meal per day is adequate (assuming protein goals are met).
Protein Pacing: Why Distribution Still Matters
While total daily protein intake matters most, how you distribute that protein can matter, especially during weight loss. Muscle protein synthesis is a temporary process that spikes after protein intake and then tapers off. Eating protein at regular intervals helps “retrigger” MPS throughout the day.
For most people, this simply means including a solid protein source at each meal. Eating three to five protein-containing meals or snacks per day can help keep MPS elevated, support satiety, and stabilize blood sugar, which is an important consideration for GLP-1 users.
That said, if appetite is very low, fewer meals can still work, provided total protein intake is met.
Best Protein Sources
Protein quality comes down to two things: how easily your body can digest it and the strength of its amino-acid profile. Amino acids are the building blocks of protein, and your body uses 20 of them to grow and repair tissue.
Nine of these are considered essential, meaning your body can’t make them on its own—you have to get them through food. There are different ways to judge protein quality, and, unfortunately, there’s no one database that stores protein quality scores. However, here are the consensus best protein sources you can consume:
- Animal proteins: Chicken breast, turkey, beef, eggs & egg whites
- Fish & shellfish: Salmon, tuna, mackerel, scallops, shrimp
- Plant-based proteins: Tofu, seitan, tempeh, lentils
- Protein-rich dairy: Milk, cheese, cottage cheese, Greek yogurt
- Supplements: Whey protein isolate, soy protein isolate, casein protein, protein bars
Ready to Build a Personalized Plan?
Discover how prescription GLP-1 medications like semaglutide or tirzepatide, combined with the strategies in this guide, may support sustainable weight loss tailored to your health needs.
Measuring Success Beyond the Pounds
If your goal is weight loss, the scale is a useful tool; it shows whether you’re generally trending in the direction you (and your doctor) want. But it shouldn’t be the only metric you rely on. There are other effective ways to measure the changes happening in your body.
Rethink the Scale
Your scale tells you whether you’ve gained or lost weight, which is helpful, but it doesn’t tell the whole story. Simply weighing yourself doesn’t account for body composition—the ratio of muscle to fat you carry—which is one of the most important markers of overall health.
Better body composition is linked to stronger bones, better metabolic health, and increased longevity. Instead of obsessing over a single number, use simple tools to track the changes you can’t see on the scale:
- Progress photos: Weekly or biweekly photos under the same lighting conditions show physical changes. The eye test isn’t always accurate, but visual changes in your body are often a sign that you’re making body composition changes.
- Waist measurements: If your waist shrinks but your weight stays the same, that’s a strong sign you’ve lost fat and maintained (or built) muscle.
- Body fat tests: Some home scales use what’s called biometric impedance to measure your body composition. It’s not a truly accurate measure, but it’s a solid reference point for whether your body composition is trending in the right direction. More accurate methods include skinfold tests and a DEXA scan, but they require other people and are usually more expensive.
- How your clothes fit: Say you don’t weigh yourself, take photos, or track your body fat, but your belt is two notches tighter, well, that’s also a “non-scale victory”. If clothes that once felt snug are now fitting looser, then that’s a sure sign that you’re losing weight.
Watch Your Health Markers
Progress can be clinical, too. Improvements in blood sugar, cholesterol, blood pressure, and other lab markers are meaningful signs that your body is getting healthier, even if the scale hasn’t budged. Especially for people using GLP-1 medications, these internal changes can happen before noticeable changes on the scale. If your bloodwork is trending in the right direction, you are making progress.
Track Strength Gains
When you’re in a calorie deficit—especially on GLP-1 medications—it’s normal to worry about muscle loss. But if your performance in the gym is improving, that’s a strong indication your muscle is sticking around. Here are a few signs to look for in the gym:
- Heavier weights: If you’re lifting more than you were a few weeks ago, you’re not just maintaining muscle, you’re likely building it.
- More reps at the same weight: Increasing from, say, eight reps to 12 reps at the same load is a textbook sign of muscular progress.
- Better technique: Lifting the same load with cleaner form, smoother reps, and improved control means you have more control over weights that once challenged you. This is likely a sign that your muscles are stronger.
- Higher work capacity: If you can get through the same workout faster or with less fatigue, your muscle endurance and strength are improving.
Body recomposition takes effort, but you don't have to do it alone. If you're considering whether a GLP-1 medication could support your journey, our quick, free online assessment can help you explore your options with guidance from licensed healthcare providers.
Frequently Asked Questions

By Andrew Gutman, NASM-CPT
Contributing Author
Andrew Gutman is a NASM-certified personal trainer and journalist with 10 years of experience covering fitness and nutrition. He’s the former fitness editor at Muscle & Fitness and was managing editor at BarBend, where he led coverage of the Olympics and World’s Strongest Man. His writing appears in Men’s Health, Business Insider, and Gear Patrol. Outside of work, Andrew trains in Brazilian Jiu-Jitsu, kickboxing, and bodybuilding—and is a proud stay-at-home dad to his first son.


